 Jennie Young’s work life is divided between being a Principal Educator (Trauma) at NHS Education for Scotland and Nurse Psychotherapist, Trauma Clinic, NHS Forth Valley. Jennie was also seconded to the Faculty of Health Sciences and Sport at Stirling University between 2013 – 2018, where she was part of a team who created an award-winning trauma-informed nurse education curriculum.
Jennie Young’s work life is divided between being a Principal Educator (Trauma) at NHS Education for Scotland and Nurse Psychotherapist, Trauma Clinic, NHS Forth Valley. Jennie was also seconded to the Faculty of Health Sciences and Sport at Stirling University between 2013 – 2018, where she was part of a team who created an award-winning trauma-informed nurse education curriculum.
My working life began as a Learning Disability Nurse over 30 years ago. I had an incredible grounding in all aspects of nursing whilst working with people with Learning Disabilities. My work led me to many different challenges, culminating in setting up the Additional Support Team at NHS Forth Valley for people displaying significant distress through behaviour, dual diagnosis and forensic issues. What I didn’t appreciate at that time was the impact of trauma, and how that was being expressed.
In 2003, I joined the Behavioural Psychotherapy service at NHS Forth Valley and immediately found myself drawn to the Trauma Clinic, which was part of the Behavioural Psychotherapy service. This had initially been developed as a response to the tragic events in Dunblane. But it has gone on to broaden its scope and reach across all aspects of psychological trauma. As Scotland’s first nurse-led trauma clinic, it was an incredible opportunity to join a dynamic and ground breaking research-based team. Almost two decades later, I still work there and it remains a progressive, dynamic team.
Although psychological trauma is a common human experience, it is too often unrecognized and untreated. It is no longer a secret that in the absence of buffers (such as supportive relationships), ‘toxic stress’ can have serious negative consequences. Psychological trauma is not confined to a single event or ‘Type 1’ trauma (such as an assault or a natural disaster), which may present as PTSD type symptoms.
In healthcare, we are often more likely to be working with people who have experienced ‘Type 2’ trauma, including serious adversity in childhood. This is often described as Complex Trauma and can include abuse, neglect, bullying or gender based violence. This can present in many ways, including attempts to cope that can themselves become harmful, e.g. substance use, obesity, self-harm, unhealthy relationships and isolation. Psychological trauma, especially of the type described above is strongly associated with physical and mental health morbidity and mortality.
To raise awareness of the realities of psychological trauma, and to help trauma-informed practice become part of the furniture across Scotland, I am currently seconded half-time with NHS Education Scotland (NES). I have a special interest in assisting my fellow community nurses acquire the skills, knowledge and understanding necessary to provide holistic, authentically person-centred, trauma-informed and responsive practice. One way it will happen is through the National Framework- Transforming Psychological Trauma: https://www.nes.scot.nhs.uk/education-and-training/by-discipline/psychology/multiprofessional-psychology/national-trauma-training-framework.aspx
Another significant opportunity to take this work forward is through QNIS’ Catalysts for Change programme. The Queen’s Nursing Institute Scotland website has all the information needed to apply for one of these project grants. I was pleased and impressed that half of the 2019/20 projects will be united under the theme of preventing, recovering from or mitigating the impacts of psychological trauma. This is broadly defined and can include a wide range of proposals growing out of the experiences and insights of the community nurses who will lead these Catalysts for Change activities. Please consider applying before 23 September, if the timing and circumstances are right for you.
The key for me was starting to see the world, our service and the people who come to our clinic through a trauma-informed lens. Over the years, five fundamental touchstones emerged:
- Trauma is everybody’s business. There is a tendency to view trauma as solely a mental health issue. The impact of trauma is far reaching and across all domains. Therefore, an understanding and response from all areas of practice is vital.
- The most important question is not ‘what’s wrong’ with this person, but rather ‘what happened’ to this person? Trauma is not just the event(s). As SAMHSA (Substance Abuse and Mental Health Services Administration) has noted, it is also the individual experience of that event, and its effects upon each person that determines the degree of trauma.
- In order to ‘do no harm’, we must understand the concept of retraumatisation. When someone has had traumatic experiences in the past, some of our practice approaches can (unintentionally) retrigger traumatic stress reactions, including anxiety, panic, ‘shutting down’ emotionally or appearing angry and distressed. Such common elements of our practice as injections, intimate examinations, firm instructions or screening tests can rekindle a past trauma.
- Trauma is not only about the presence of several negatives, but also about the absence of the positives that enable resilience and recovery. Helping people discover and build upon their inner strengths and individual qualities is at least as important in the long run as professional assistance to cope with adversity.
- Trauma-informed practice is not about ‘those people’. Psychological trauma is a near universal human experience, from which community nurses (and all other professionals) are far from exempt. In fact, for many of us, our own experiences of trauma may have kindled the desire to help others Self-awareness and self-care are crucial to becoming a truly trauma-informed, clinically-effective community nurse.
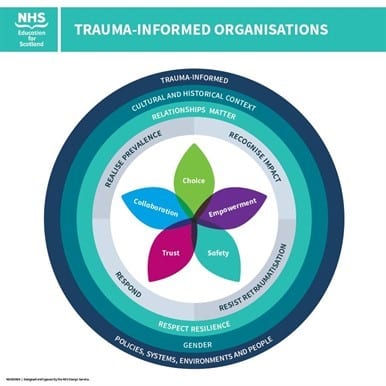
The graphic below illustrates the ‘big picture ’in professional and organisational terms.
Perhaps the most important truth to remember as community nurses is that we occupy an unusual (and sometimes unique) position of power and influence in relation to the people with whom we work.
Building and maintaining mutually-beneficial relationships are essential to trauma-informed practice that ‘works’ for all concerned. Few other professionals have the privilege and the opportunity to develop relationships as strong and enduring as those available to many community nurses.
I wish you the same good fortune, great mentors and continuous learning that enabled me to grow my trauma-informed, community nursing ‘wings’ – one feather at a time.